|
A
peer-reviewed electronic journal published by the Institute for Ethics and ISSN
1541-0099 29(1) – May 2019 |

Can we make wise decisions to modify
ourselves?
Some problems and considerations
Rhonda Martens
University of Manitoba
Journal of Evolution and Technology - Vol. 29 Issue 1 – May 2019 - pgs 1-18
Abstract
Much of the human enhancement literature focuses on the ethical,
social, and political challenges we are likely to face in the future. I will
focus instead on whether we can make decisions to modify ourselves that are
known to be likely to satisfy our preferences. It seems plausible to suppose
that, if a subject is deciding whether to select a reasonably safe and morally
unproblematic enhancement, the decision will be an easy one. The subject will simply
figure out her preferences and decide accordingly. The problem, however, is
that there is substantial evidence that we are not very good at predicting what
will satisfy our preferences. This is a general problem that applies to many
different types of decisions, but I argue that there are additional complications
when it comes to making decisions about enhancing ourselves. These arise not only
for people interested in selecting enhancements but also for people who choose
to abstain.
1. Introduction
Alexis Madrigal, an
American journalist, decided to implant a magnet under the skin of his
fingertip. He came to this decision while interviewing bodyhackers
for an article he was researching. The bodyhackers
spoke with such enthusiasm about how having magnets under their fingertips
opened up new sensory worlds that Madrigal decided to try it for himself. Once the novelty wore off, he discovered that he
did not like having a magnet under his fingertip all that much. He reports that
he sometimes worried about the possibility of infection, and that he would likely
get the magnet removed at some point (Madrigal
2016).
The decision whether
or not to install a magnet under the skin seems a minor one, akin to getting
ears pierced. There are, however, more substantial interventions we can
undertake to change our abilities or our bodies (e.g., Neil Harbisson
implanted a device in the bone of his skull that allows him to hear colors (Jeffries 2014)), and it is likely that more
profound decisions will face us in the future. Many authors discuss the safety
of future possible enhancements (Chatwin et al.
2017; Torres 2016; Douglas 2015; Bostrom and Sandberg 2009), their
influence on our society (Crittenden 2002;
Fukuyama 2003), and their potential influence on our moral selves (Archer 2016; Agar 2014; Persson and Savulescu 2013;
Sandel 2009) and our sense of self (Edelman
2018, Coeckelbergh 2011, Cabrera 2011, Sandel 2009). In what follows, I
will argue that, even if we can successfully address these issues (a tall order
in some cases, but reasonably easily met in the case of Alexis Madrigal’s
choice), we still face the problem that we cannot always know whether our
decision to modify or not modify ourselves will satisfy our preferences.1
Madrigal discovered only after the fact that he preferred the sensation of an
unmodified finger to one with a magnet installed. Furthermore, this problem
faces not only those who are interested in bodyhacking
and enhancement, but everyone, including the abstainers. Once a modification is
contemplated and considered, abstaining is still a choice made without
sufficient information to know that it is the best route to satisfying our preferences.
The decision problem I
am identifying is known in the decision theory literature as making a decision
under uncertainty. After a few preliminaries, I will give a brief,
non-technical description of the problem of deciding under uncertainty. Then I
will present five routes for addressing uncertainty. The bulk of this article
will examine these five routes and the ways in which they can and cannot be
used to make wise decisions about enhancements and body modifications (I use
the term “modification” to signal that in some cases we might want to change
ourselves without making ourselves “better” in some sense). While it is true
that we normally have difficulties figuring out which choices will satisfy our
preferences, I will consider the specific problems that face us when we decide
whether to adopt or reject getting modifications.
Toward the end, I will
consider whether the decision difficulties for modifications are on a par with
other momentous decisions we face. For example, people routinely decide whether
to get married, or to have children, or to pursue a certain career, and we make
all these decisions without sufficient information to know with certainty that
we have made the right choice. I will argue that, for certain types of
enhancement or modification decisions, the lack of information is a more
serious problem than for these other momentous decisions. To clarify, the thesis
is not that we cannot make rational decisions about modifying ourselves. We
can, if we define “rational decisions” as decisions that follow some reasonable
set of decision-theoretic rules. The thesis is also not that we cannot make the
right decision, if this means the one
that leads to the best outcome. It is, after all, possible even for foolhardy
decisions to lead to lucky outcomes. Instead, the thesis is that, when we are
dealing with an information gap, the extent to which rational decisions track
right decisions weakens, and the information gap for certain modification
decisions is larger than for other types of momentous decisions.
My focus here is on
decisions we make on behalf of ourselves, as opposed to decisions we might make
on behalf of others. I will also concentrate on decisions about actions that
are neither morally required nor forbidden. Installing magnets under the skin
seems to fall under this category, and is a relatively minor decision. Note,
however, that non-obligatory, permissible actions can be quite profound in
their consequences or implications. For example, in 2006 the Guardian reported on a case where a
man’s penis was damaged beyond repair in an accident. He opted for a penis
implant, which seems both non-obligatory and permissible. The implant was
medically successful. Nonetheless, surgeons removed the transplanted penis two
weeks later because the recipient and his wife could not psychologically accept
it (Sample 2006). I think it is easy to
imagine why the man consented to the transplant surgery, and easy to imagine
why the results would be sufficiently psychologically disturbing to warrant the
removal of the transplant. It would also be understandable if a year or two
down the road the man regretted his decision to remove the transplanted organ.
This case points to the difficulties in making decisions about how we might
modify our own bodies.
When decisions made on
behalf of oneself are about permissible, non-obligatory actions, many of the
reasons we have for them will be based on whether the decision is likely to
satisfy our personal preferences. These types of reasons are subjective, and they
vary from individual to individual. I will follow L.A. Paul (2014, ch. 2) in calling these types of reasons
first-personal. While it is true that, for some decisions, more objective, or
other-directed, reasons might prevail (for example, we might prefer to remain
unmodified, but might decide to improve our intelligence in order to increase
the odds of discovering a medical treatment that would save the lives of many),
a wide variety of decisions might reasonably involve mostly first-personal
reasons. I will focus on decisions based on
first-personal reasons in this article, although there are further interesting
conversations to be had about decisions involving a mix of first-personal and,
in the relevant sense, objective reasons (Martens 2016 briefly touches on this
subject, although not in the context of decision theory).
Paul argues that, when
the reasons for making a decision are first-personal,
what we need to know is the “what it is like for me,” or the “what it is like
for the agent” (the WIILFA) (Paul 2015b, 808–809).
The WIILFA has two components. The “what it is like” refers to lived
experiences, a kind of “thisness” of the now. The
“what it is like” cannot be fully communicated from one person to another. For
example, there is a difference between being told, “You will hear an extremely
unpleasantly loud noise,” and actually experiencing that noise (Hsee, Hastie, and Chen 2008, 233). The “for me” or “for the
agent” part signals that what matters in making a first-personal decision is
whether the agent will prefer the outcome, rather than whether people in
general, or even people similar to the agent, will prefer the outcome. Some
decisions are going to be more WIILFA-dependent than others. For example, the
WIILFA of “it feels great to be smarter” seems less important than the WIILFA
of “it feels great to be able to hear colors.”
2. Rational decisions
The standard procedure
for making a rational decision involves making a calculation based on the
following pieces of information:
1) The possible ways the world could be (the state) that are relevant
to each choice.
2) The probabilities that the possible states will occur should the
agent make that choice.
3) The outcomes based on the states.
4) The expected values of the outcomes.
The decider will often
lack full information about the above four pieces of information. Furthermore,
lacking information about the first will influence the other three. Before we get
to problems about lacking information, let’s consider a relatively simple
example about buying a lottery ticket (Table 1). The choices are on the
left-hand side of the table. They are: buy ticket with number x; do not buy
ticket. The states are in the top row of the table. They are: Ticket number x
wins; Ticket number x does not win. The outcomes are the results of the choice
and the states, and are numbered in the table from best expected value to worst
expected value.
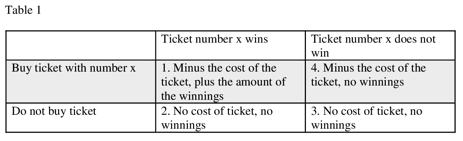
If we do not consider
the probabilities of each state occurring, then buying the ticket seems the
rational choice because it can give us the highest value outcome. Obviously,
then, we should consider the probabilities. While the expected value of winning
a lottery is high, the probability of winning is low, and so we are more likely
to end up with the worst outcome (outcome 4), rather than the best, if we buy
the ticket. Unless we derive an additional value out of purchasing the lottery
ticket (for example, coworkers might purchase lottery tickets together as a
kind of community-building activity), we should not purchase it. (Outcome 2 can
become the worst outcome if the decider knows she could have bought the winning
ticket. Suppose, for example, she normally selects a specific sequence of
numbers but opts out in the week that those numbers win. Then the decider gets
to add “deep regret” to outcome 2.)
Now let us consider
whether I should get a magnet implanted under my fingertip (see Table 2).
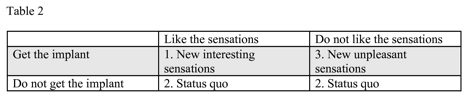 This is a simplified table. For example, I have
excluded the possible state where my finger gets infected. I have also excluded
a category for states that we have not anticipated. I want to note two things.
First, the states in question are experiential and subjective (whether I like
the sensations). Second, since I have never had an implant, the decision is
about whether to have a novel experience. The novelty and subjectiveness
contribute to my not knowing the probability of whether I am the kind of person
who will like the sensations or the kind of person who will not. This implant
decision problem is different from the lottery case. In the lottery case, we do
not know in advance which state will occur (winning or not winning), but we do
know that the probability of winning is very low. We know the probabilities of
the states in the lottery case, but not in the implant case (or, we might
subjectively assign probabilities with a low level of confidence in those
probabilities, but I will not get into such technical issues here). This lack
of knowledge will impair our ability to choose the act most likely to lead to
the best outcome.
This is a simplified table. For example, I have
excluded the possible state where my finger gets infected. I have also excluded
a category for states that we have not anticipated. I want to note two things.
First, the states in question are experiential and subjective (whether I like
the sensations). Second, since I have never had an implant, the decision is
about whether to have a novel experience. The novelty and subjectiveness
contribute to my not knowing the probability of whether I am the kind of person
who will like the sensations or the kind of person who will not. This implant
decision problem is different from the lottery case. In the lottery case, we do
not know in advance which state will occur (winning or not winning), but we do
know that the probability of winning is very low. We know the probabilities of
the states in the lottery case, but not in the implant case (or, we might
subjectively assign probabilities with a low level of confidence in those
probabilities, but I will not get into such technical issues here). This lack
of knowledge will impair our ability to choose the act most likely to lead to
the best outcome.
The problem of making
decisions without knowing with confidence the probabilities of the states is
well known in the decision theory literature, with many approaches offered (for example, Wald 1950, 18; Hurwicz 1951; Savage
1972, ch. 9; Skyrms 1990, 112–14 ; Weirich 2004, ch. 4; Stoye 2011; Buchak
2013, ch. 1). For example, one could follow the rule (the maximin rule) where one makes choices to avoid the worst
outcome, which in this case is outcome 3 (get the implant + do not like the
implant = new unpleasant sensations). Then I should not get the implant. A
different rule would have me considering whether I am risk-averse or
risk-adventurous, and then make my selection accordingly. Since I am
risk-averse, I would make the choice to avoid the worst outcome (outcome 3).
Alexis Madrigal seems more adventurous, at least from his telling of the story,
and he justified his choice because he had an interesting learning experience. According
to this rule, the decision to get the implant is irrational for me, but
rational for Madrigal given our different attitudes toward risk (and given that
the risks associated with implanting magnets are quite low). Notice that these
decision rules are to be applied at the time of making the decision. Below I
will discuss strategies for gathering information prior to the time of making the decision.
If we merely apply
some reasonable decision rule when operating under an extreme lack of
information about the probabilities of the states, then we have reasons for our
decisions. Making a reason-based decision is not the same thing as making the
right decision. The right decision is the one that actually brings about the
best outcome. When operating under an extreme lack of information, a wedge is
driven between reason-based decisions and right decisions. In this context,
reason-based decisions might not perform much better than a guess. Notice that
this problem is symmetrical in the following way. A rule that prioritizes the
status quo is no more likely to track the best outcome than a rule that
prioritizes exploration. When facing modification decisions, we are no more
likely to get it right if we reject the modification than if we adopt it. It is
possible that if we could experience the WIILFA of the modification in advance
of making the decision, we might conclude that the status quo is entirely
unacceptable. The reverse is also possible. Neither transhumanists
nor bioconservatives have an edge here.
Not all is lost.
Sometimes we can take steps to reduce the amount of uncertainty. Here I am
concerned with applied rather than theoretical decision theory, so the goal is
to collect strategies that can be used by real agents rather than ideal agents.
Several authors (Burnett and Evans 2016;
Krishnamurthy 2015; Dougherty, Horowitz, and Sliwa 2015; Pettigrew 2015; Paul
2014, 2015a, 2015b, 2015c; Weirich 2004) focus on realistically usable
strategies. With the exception of the first strategy surveyed below, these
differ from rules like the maximin rule in that they concern
how we should gather information or frame the decision. These are strategies
for preparing for a decision prior to applying a decision rule. I will survey these
five strategies before applying them to decisions about body modification. Not
all of these strategies will turn out to be good strategies for making
decisions about body modification, and all of them will have limited applications.
3. Five strategies for dealing with uncertainty
3.1 – High need or low cost
The idea here is that,
while we face a lack of information about the WIILFA of the novel experience,
we may still have enough information to make a choice. In the high need case,
the costs of not changing are high enough to motivate trying a novel
experience. For example, having a currently untreatable fatal disease could
make it rational to try an experimental treatment despite a lack of information
about effectiveness or safety (for an
introduction to dominance, see Whitmore and Findlay 1978, 24–27). In the
low-cost case, while we might not know whether we will prefer the WIILFA of the
novel experience, the costs of trying are low enough to be worth finding out.
The low-cost case can be buttressed by a decision rule focused on avoiding
regret. The strategy of appealing to high needs or low costs clearly has
limited applications, as will be discussed in section 4.
3.2 – Curiosity
We could justify
trying the novel experience on the grounds that we value discovering what it
will be like. This way, at least one of our preferences – the preference to
discover what it will be like – will be satisfied regardless of what the other
aspects of the experience will be like. This is a reframing strategy proposed
by Paul in response to the failures associated with the next option (Paul 2014, ch. 4). As we shall see in section
4, the curiosity option has extremely limited applications. Furthermore, the
adventurous might find themselves regretting their adventures if the outcomes
are bad enough.2
3.3 – Imagination
We could use our
imaginations to try to determine what the novel experience will be like for us.
Paul refers to this as a natural approach, which we use for many types of
decisions (Paul 2015c). For example, when
deciding on purchasing a new home, one might begin the decision process by imagining
living in the home.
Paul also insists that
using our imagination is a necessary approach when decisions depend on the
value of the WIILFA for our future selves undergoing the experience.
Imagination, Paul argues, is the only way to grasp what our unique future
selves will be like because empirical studies can only be about other people
who may or may not resemble our future selves (2015b, 448–87). The problem, which Paul acknowledges and
will be elaborated on in section 4, is that our imagined future self is not
likely to resemble our actual future self in the way that we need.
3.4 – Prototyping
Weirich (2004, 27) points out that rational agents will not
simply rest content with applying decision rules to the information they have,
but will collect new information whenever possible (a sequential versus a
static approach to decision theory). He highlights the strategic value of
making a series of decisions, each of which leads to acquiring new information
that influences the next decision. In their self-help book on making decisions,
Burnett and Evans offer similar advice from a less academic perspective (2016, ch. 6). They recommend prototyping, which involves seeking
out lower risk experiences that are similar to the novel experience we are
considering trying. For example, if we want an RFID chip implant in our hands that
will allow us keyless entry into our homes, we could try the chip on a wearable
device first. Krishnamurthy (2015) offers a similar suggestion when she argues
that we can obtain information about what it will be like to be a parent by
spending lots of time caring for children. This involves an argument by analogy, that the prototyped experiences we have had in the
past are sufficiently similar to the experiences we will have in the future if
we make the higher risk decision. This strategy and the next are the most
promising routes, although their limitations will be discussed in the next
section.
3.5 – Collecting empirical data
The most common advice
in the literature is to collect more information about the probability of the desired
states by consulting empirical studies (quantitative or qualitative) of others
who have already made the same decision (Krishnamurthy
2015; Dougherty, Horowitz, and Sliwa 2015; Pettigrew 2015). If we are
considering a body modification, we should find out if others who have already
tried the modification found it to be a valuable experience. This also involves
an argument by analogy, to the extent that we are relying on those people being
similar to us in relevant ways. This is not a watertight argument, however. After
all, they might prefer the experience while we do not.
Note that strategies
3, 4, and 5 (imagination, prototyping, and collecting empirical data) involve
trying to gather information on the probabilities of whether the subjective
experiences will be valuable to us. In other words, the problem of uncertainty
is addressed by reducing the level of uncertainty. Strategy 2 (curiosity) does
as well, but in a different way. It involves shifting focus from future states including
or not including the WIILFA to states about discovering or not
discovering the WIILFA. The agent might not know whether she will like the
WIILFA, but she will have information about whether she values discovery or is
risk-averse.
Strategy 1 (high need
or low cost) does not involve basing justification on an approximation of the
expected value of the WIILFA of the novel experience at all, but on either the
known bad expected value of the WIILFA of the known outcome or the known low
risks of the novel option. Whatever might be the expected value of the novel
WIILFA, it stands a good chance of being better than the WIILFA of the known
outcome, or in any event it is unlikely to be bad enough to avoid.
4. The main argument
It is now possible to
state an outline of the argument of this article:
1) In order to be reasonably confident that our decisions will satisfy
our first-personal preferences about the WIILFA, we need to reduce sufficiently
the amount of uncertainty associated with a decision. This applies equally to
the decision to stay the same as it does to the decision to change or enhance
oneself.
2) For many people, and for certain types of modifications, the above
five strategies are either inadequate or unavailable for reducing sufficiently
the amount of uncertainty associated with a decision. (This is especially likely
in the early stages of modification research. If modifications come into
widespread use, we will be presented with different problems, discussed below.)
3. Therefore, if the above
five strategies are the only routes for sufficiently reducing uncertainty, then
for many people, and for certain types of modifications, a reasonable amount of
confidence that decisions will satisfy first-personal preferences cannot be
obtained.
It is worth noting
that we are currently facing this problem. I have already not installed
magnets under my fingertips many times. If you are like me, then you will also
have made many such decisions without a great deal of thought.
One
obvious vulnerability of the
argument, implicit in the wording of its conclusion, is the possibility of some
strategy not in the list of five mentioned above. Any further justification
strategies will make for interesting discussion at another time. I cannot deal exhaustively
with the issue on this occasion, although at the end of the article I will
speculate briefly on routes we might take. Meanwhile, the bulk of what follows
will focus on justifying premise 2. I will examine each of the suggested
strategies, in order to show why they do not always apply.
4.1 – High need
or low cost
It is possible to make
rational decisions when the outcomes of a novel course of action are unknown if
the outcomes of the other course of action are known to be sufficiently worse.
For example, in the 1980s, many people infected with the human immunodeficiency
virus (HIV) were willing to try experimental drugs because the known outcomes
of not trying the drugs were severe.
It would be far too
quick to rule out this justificatory strategy for enhancements on the grounds
that enhancements are not treatments. Aside from the
oft-noted blurry boundary between enhancements and treatments (see, for
example, Agar 2014; Lara 2017), sometimes enhancements are still solutions to
problems. This justificatory strategy is not limited to life and death
situations. All that is needed is enough information to be able to conclude
reasonably that, whatever the outcomes might be from the novel course of
action, they are very likely to be better than those of the non-novel course.
I have grouped the
high-need reason together with the low-cost reason because they both depend on
a proportional bar of risk. If the possible risks of the novel action are
reasonably low, then the problem it is intended to solve does not need to be
severe. Consider the magnet case. While it is novel, and we might be in the
dark about whether we will like the insertion of a subcutaneous magnet, we
still have a pretty good idea of some of the risks. They are fairly low. We
know, to use an absurd example, that installing magnets under our skins will
not turn us into frogs. Since the range of possible outcomes of installing a
magnet are not extremely bad, the problems that magnets could solve also do not
need to be extreme. They only need to outweigh the range of possible negative
outcomes. Let us consider a few examples of enhancements that are solutions to
problems.
Amal Graafstra had the problem
of leaving his keys in his office and locking himself out. He solved his
problem by installing an RFID chip implant under the skin of his hand that
unlocks his door. Now he does not lose his keys anymore (Graafstra 2013).
Neil Harbisson is a visual artist who was born completely color
blind. Nonetheless, he wanted to work artistically with colors, so he installed
a device that is fused to his skull and allows him to hear colors (Jeffries 2014).
In an article on bodyhacking published in the New York Times, Hylyx Hyx
is quoted as saying, “I’m used to having weird feelings about my body . . . I
use ‘they’ pronouns. I don’t care about most of my meat, so this is a way to
have control over a part that I chose” (Hines
2018). One way to interpret Hyx is as
expressing a lack of connection with their body, and a desire to control it.
Through body modification, Hyx can now control and
connect to their body.
Hylyx Hyx also stated that they
are a “submissive for science” (Hines 2018). One interpretation of this claim
is that Hyx is willing to be an experimental subject.
It is possible that such experiments could lead to treatments that address not
the high needs that Hyx has, but needs that others
have. This, however, is not a common motivation.
Liao, Sandberg, and Roache (2012) argue that if we enhance ourselves
and our offspring so that we consume fewer resources and are more
intelligent and ethical, we might be able to find a solution to the pressing
problem of climate change.
Back
to the HIV case. It would not
normally be rational to try an untested drug if another known effective drug
were available. In the above four examples, there are alternative solutions to
the problems. Graafstra and Harbisson
could use wearables. Hyx could
stick to piercings, tattoos, or diet plus the gym to control their body. For
the problem that Liao, Sandberg, and Roache raise, our
respective governments could better incentivize good environmental behaviors on
our part (which seems a more likely successful route than incentivizing that we
modify ourselves and our offspring).
It is possible that Graafstra, Harbisson, and Hyx would find my alternative proposals unacceptable. They
could, for example, have deep identity-based reasons for why implants, even
implants with potentially negative consequences, are a more palatable way to go
than the alternatives. I do not know them personally, so I cannot say what
their reasons are, but it is certainly conceivable, and even likely, that some
people might have deep identity-based reasons for wanting to modify their
bodies in certain sorts of ways, even if Graastra, Harbisson, and Hyx themselves do
not. For an identity-based reason to count as a high enough need to swamp other
considerations, it would need to be similar to what many trans*3
people experience when deciding whether or not to transition. Rachel McKinnon offers
a version of this decision-making strategy when she points out that, while
trans* people might not know what it will be like to transition, they are often
faced with dire situations if they do not. To support this, she cites studies of
high suicide rates of trans* people (McKinnon 2015, 423–24). Similarly, White
cites studies of the suffering of people with Body Integrity Identity Disorder
who are prevented from obtaining elective amputation for the purposes of
aligning their bodies with their identities (White 2014, 226).
Even if, however, we
can successfully argue that identity expression through body modification is
important enough to swamp the possible negative outcomes, it also seems likely
that this method of justification will be available only to some people. Many others
will not feel driven by identity reasons to expand their abilities or modify
their bodies. Thus, to the extent that the identity threat argument works, it
will work only for some. Furthermore, many of the enhancements and
modifications that we might consider are not solutions to any problem at all. Therefore,
the high need/low cost approach is a justificatory strategy with limited
application.
4.2 – Curiosity
The adage, “Fools rush in where angels fear to tread” is one description
of what happens when people base a decision to try the novel on curiosity. Here
is another description. Paul proposes that we can reframe the decision problem
in a way that permits a rational decision to be made. The idea is this. Instead of trying to ascertain which option will
increase first-personal value based on an unknowable WIILFA, we might base the
decision on whether we value finding out the WIILFA. For example, if we value
knowing the WIILFA of having magnets under the skin of our fingertips, we will
satisfy that value regardless of what the WIILFA turns out to be (Paul 2014, ch. 4). In Alexis Madrigal’s case,
given the tone of his report, it seems that he valued having the implant
experience for the purpose of finding out what it would be like, even though,
in the event, he did not particularly care for the what-it-was-like. (We can
use this reframing strategy not just for values such as a discovery preference,
but also for values such as controlling one’s body.)
We can also use this
reframing strategy for rejecting the
novel experience. For example, it is quite reasonable to value not finding out the WIILFA of
age-related cognitive decline, so taking a preventative drug to avoid having
that discovery is rational.
There are at least two
ways in which the valuing discovery option is limited. First, for certain types
of decisions, it counts as a terrible reason. Consider Paul’s stock example of
choosing to have a child for the first time. Having a child for the sake of wanting
to find out the WIILFA seems incredibly flippant. This level of flippancy might
be reasonable when it comes to more trivial decisions like installing magnets
or RFID chips under the skin, but not for deciding to have a child or deciding
to take on a more profound enhancement. The level of risk matters here. Also,
in the case of deciding to have a child, other parties are deeply affected by
our decision. (Interestingly, the flippancy seems to disappear when we consider
the decision to not enhance or to not have a child. Wanting to not find out the
WIILFA seems acceptable here.)
Second, only a
relatively small number of people will be able to make use of the curiosity-justification
strategy. Basing a decision on valuing discovery is available to those for whom
wanting to find out the WIILFA is a sufficient reason to adopt an enhancement.
It is also available to those for whom wanting to not find out the WIILFA is a sufficient reason to avoid an
enhancement. Basing a decision on valuing discovery is not available for the
following two groups: those for whom these wants are not sufficient (e.g., I am
kind of curious about having an RFID chip implant, but not enough to override
my concern about uncertainties about the WIILFA); and those who do not have
wants either way about discovering the WIILFA. Let us explore the latter point.
There is a distinction
between wanting to not find out the
WIILFA, and not wanting to find out the WIILFA. The first involves an active
desire to avoid learning about the experience. For example, I have an active
desire to avoid finding out what it feels like to jam a pencil into my hand.
The second involves the absence of an active desire. For example, I do not have
any desires one way or the other to find out the WIILFA of having arms that are
1 centimeter longer than they currently are.
While it seems pretty
clear that the bodyhacking movement is driven forward
in part by curiosity (along with other desires, such as controlling one’s body)
– and so, many bodyhackers can avail themselves of
this justificatory strategy – the bodyhacking
community is relatively small. It seems very likely that many people will fall
into the categories of either not having a sufficient desire to discover/avoid
finding out the WIILFA or not having a desire at all about the discovery aspect
of enhancement. These people, then, are still faced with the problem of
justifying their decision either to try or to avoid the novel enhancement.
4.3 –
Imagination
A large body of
literature in psychology shows that we are terrible at predicting whether, or
how much, we will prefer an experience (Wilson and Gilbert 2005; Gilbert et al.
2009; Walsh and Ayton 2009). We are terrible at this even when the predictions
in question involve events we have experienced many times in the past. For
example, if we are still full from the last delicious meal, we tend to
underestimate how much we will enjoy the next delicious meal. Yet we have gone
through the process of moving from satiety to hunger many times in our life.
Given this, we can expect to be terrible at predictions about the
first-personal values of novel experiences. As some authors have previously pointed
out, future research on human enhancements might take us in directions that
boggle our imagination (Mihailov and Dragomir
2018).
It is worth taking a
few moments to review one of the identified errors we tend to make when trying
to ascertain whether we will prefer a new experience, and whether the price we
pay for that new experience is suitable. Forewarned is forearmed. We tend to
overestimate how much we will react to a future event (Wilson and Gilbert 2005). To use Hsee,
Hastie, and Chen’s (2008) example, when we first move into a larger home, our
initial feelings of pleasure will be stronger at the start. Later, however, we
will adjust to this larger home, and the intensity of the pleasure will
decrease. Hsee, Hastie, and Chen refer to this as the
distinction between acquisition and consumption. When deciding whether or not
the larger home is worth the greater expense, we often make the mistake of basing
our decision on the prediction of the acquisition experience rather than the
consumption experience.
Similarly, when
considering modifying the body, we might make the mistake of basing our
assessment on a prediction of the acquisition experience rather than the
consumption experience.
4.4 – Prototyping
If the problem of
uncertainty arises because we do not have past experiences that are
sufficiently similar to the future experiences we are considering, we may make
lower risk decisions that give us information about those future experiences.
Earlier, I gave examples such as wearing an RFID chip on a ring before
implanting it in the hand. For another example, Neil Harbisson,
prior to fusing a device to his skull that allows him to hear colors, wore a prototype
that strapped onto his head. This allowed him to gather significant information
on whether or not the device worked, and whether or not he could learn the
color-to-sound language (Stix 2016).
Prototyping has its
limits. One feature Harbisson could not prototype was
the WIILFA of having the device fused to his skull. Another feature that cannot
be prototyped is the long-term WIILFA. As previously mentioned, there is a
difference between the acquisition experience and the consumption experience,
and this difference matters.
Other enhancement
choices might not be suitable for prototyping at all. For example, it is
difficult to imagine how one would prototype being substantially smarter (a
little bit smarter, yes, but substantially smarter is more difficult).
4.5 – Collecting
empirical data
When making decisions, it can be useful to find out how other people
value the outcomes of their choices. We could talk directly to people about
their experiences, or read the narratives contained in qualitative studies, or
look at the results of quantitative studies. For this approach to provide us
with information about the probabilities of outcomes that satisfy our
preferences, two conditions must be met. First, there must be people who have
already made the decision in the past. Second, those people must be
sufficiently similar to us in relevant respects for the information about their
experiences to be predictive of ours. Relevant dissimilarities will weaken the
argument by analogy.
Let us consider three stages. Stage 1 is where nobody has yet tried the
modification. Stage 2 is where only early adopters have tried it. Stage 3 is
where the modification is widely used. Obviously, the stages will not, in
practice, be sharply delineated. Nonetheless, the question remains. How do we
get from Stage 1 to Stage 2, and from Stage 2 to Stage 3?
When moving from Stage 1 to Stage 2, the first condition cannot be met.
We cannot find out how others have valued the experience because nobody, to
date, has had the experience. Early adopters will need to make use of some
other method of justification. To quickly review, the high risk or low cost
strategy requires either that the status quo be high risk or the modification
be low cost. There will be some modification decisions that do not fall into
either of these categories. Valuing discovery for its own sake might be
appealing to early adopters, but again, the strength of the desire for
discovery needs to increase proportionately with the risk of the modification. Imagination is very inaccurate, and pretty much a
non-starter. Prototyping is useful, but only certain aspects of the novel
experience can be prototyped.
What are we left with? Here are three ways to move from Stage 1 to Stage
2:
1) Some people might adopt early because
their modifications are also treatments.
2) Those with a high desire for discovery might
move us from Stage 1 to Stage 2.
3) Those who make decisions without giving
them much thought might also show up in the early adoption crowd.
It is interesting to think that, in moving toward a posthuman
future, we might be relying on thoughtless behavior. As a quick aside, however,
thoughtless decision-making can sometimes be beneficial. I imagine that many
can identify with the claim that, had we given enough thought to certain
decisions (e.g., having a child or training to become a professor), we might
not have made those decisions, but we are nonetheless glad that we did.
When we move from
Stage 2 (early adopters only) to Stage 3 (widespread use), we now have people
who can report on their experiences. The question is whether early adopters are
sufficiently similar to late adopters to support an argument by analogy. Since
we are focusing on decisions that are based on satisfying preferences about the
WIILFA, what matters is whether early adopters are sufficiently psychologically similar to late adopters.
Physiological similarity between the two groups is important for establishing
medical safety and effectiveness, but psychological similarity is needed to
support the claim that, because the modification satisfied the preferences of
the early adopters, it is likely to satisfy the preferences of the late
adopters. I will argue that there are roadblocks to establishing similarity in
preference sets between the two groups. These are not insurmountable, but they
are cause for concern. We will begin with general problems on reports of the
WIILFA, and then move to problems more specific to modifications.
The first general
problem has to do with interpreting other people’s reports of their WIILFA. Hsee, Hastie, and Chen observe that, while we can use other
people’s reports to provide information, information is “cold” while
experiences are “hot.” There is an important experiential element that does not
get communicated (Hsee, Hastie, and Chen 2008, 233).
The second general
problem is with how people report on their decisions. People tend to
rationalize decisions after the fact for a variety of complicated psychological
reasons (Mather and Johnson 2000; Mather, Knight
and McCaffrey 2005; Stoll Benney and Henkel 2006). This reduces the
reliability of testimonials. On the plus side, the tendency to rationalize
makes it likely that, whatever future decisions we make, we are likely to rate
them more positively than, perhaps, we should.
For problems more
specific to modification decisions, the reasons early adopters have for their
decision might be different from those of late adopters, and these differing reasons
might reflect different preference sets. Consider the early adopter who selects
the modification as a treatment. One significant preference is to be relieved
of the condition being treated. For the early adopter who selects the
modification out of a sense of adventure, preferences for discovery, and even
risk, will be salient. The thoughtless early adopter might have a positive
attitude toward risk, at least with respect to the selected modification
(although there can be many reasons for thoughtlessness). In sum, the early
adopters might include some people who are merely thoughtless, but others are
likely to have relevantly different preferences from the late adopters. One question
that remains is whether these different preferences influence earlier and later
groups’ perceptions of the WIILFA.
There is data to
suggest that the context in which a decision is made influences the decider’s
perception of the experience and the extent to which it satisfies preferences.
For example, if a Positive Experience 2 follows another Positive Experience 1,
we are inclined to rate Positive Experience 2 less highly than we would if it
had followed Negative Experience 1 (Kahneman 1992).
For someone selecting a modification as a treatment, and assuming the treatment
is successful, we have a positive experience following a negative one. For
another example, if a decision leads to the satisfaction of a goal, we tend to
rank the experience more highly than if the decision leads to failing a goal,
even if the actions and outcomes are the same (Heath, Larrick,
and Wu 1999). For those motivated to modify out of a sense of adventure, this
type of framing could influence reports of preference satisfaction.
It is striking that,
given the identifiable differences in preferences between late adopters and those
early adopters who are motivated either by needing a treatment or by a desire
for discovery, the most suitable group for building an analogy between early
and late adopters is the sub-set of early adopters who acted thoughtlessly. The
thoughtless group is more likely to be diverse, since there can be many reasons
for acting without thought. One issue that will matter is whether the
thoughtlessness is global or local. If it is global, then it is hard to see how
late adopters can trust the reports given by the thoughtless.
To be sure, the
decider and the reporter (i.e. the early adopter) can keep these factors in
mind. The reporter can be careful in how she articulates the nature of her
experiences. The decider can sift through this information with awareness of the
roles that psychological biases might play. The late adopter does not have
perfect information, but the early adopter’s report gives him more information
than he had in Stage 1. In assessing this, the late adopter needs to be aware
that the differences between early adopters and late adopters weaken the
analogy between their respective experiences. How much this matters depends on
the magnitude of the risk if one makes the wrong decision. It also depends on
just how different the late adopter is from the early adopter. Realistically,
attitudes to early and late adoption will come in degrees. We might have
early-early adopters who provide reasonable information for early adopters, and
then the early adopters can provide reasonable information to early-late
adopters. And so on. This would be a gradual rolling out of inferences. That
said, in the early stages of Stage 2, the late-late adopters will
still have a significant information gap. I emphasize again that this is a
problem not just for those considering adopting a novel modification, but also
for those who are not. Failing to make a decision and deciding to avoid an
experience are still choices.
We also need to
consider the problem in moving from Stage 2 to Stage 3 in the context of
certain transhumanist philosophies. Neil Harbisson and Moon Ribas,
co-founders of the Cyborg Foundation, articulate a vision of a world in which
people design their own modifications in keeping with their specific desires
about how they want to interact with the world (Harbisson
and Ribas 2018). Clearly, on this vision, if we design a unique
modification, we will not have access to information about how others have
experienced it. I should note that Harbisson and Ribas recommend prototyping on their website.
5. Concluding remarks
In an article about
the ethics of human enhancement, Norman Daniels recalls an old joke about a
traveler asking for directions of a farmer. The farmer, after considering a
variety of routes, says, “You can’t get there from here.” Daniels’ point is that
we cannot ethically and safely get from our current world to one where
modifications are profound and widely used (Daniels
2009, 38–41). My point is less emphatic. If we want to get from here to
there while making informed decisions about whether the modifications will
provide us with WIILFAs that satisfy our preferences, we will encounter
significant roadblocks.
It might seem from the
foregoing that I am recommending a bioconservative position.
I am not, and these are some reasons why I am not. As already mentioned,
neither the bioconservative nor the transhumanist has the edge on increasing the odds of making
the right decision (the one that will yield the best WIILFA). Furthermore, if
we think that we can avoid this decision problem by simply avoiding research
into enhancement and modification techniques, then we
are mistaken. Avoiding research is itself a potentially mistaken choice.
Finally, and this is more of a confessional comment than anything else, I am
personally enthusiastic about the possibility of a posthuman
future such as envisaged by transhumanists. The
problem is that the future I enthusiastically imagine is one with all the bugs
and decisions already worked out, and I do not know how we can get from here to
there. I applaud Hylyx Hyx
for their willingness to be a “submissive for science” (Hines 2018), but I personally am not willing to go down that road.
I think that Ronald Dworkin put his finger on why the prospect of new human
enhancement techniques is so troubling. Dworkin, in
trying to sort out what the reasons might be for the “playing God” objection to
human enhancement, observes that when scientific developments present us with
choices we did not previously have, our views on ethics and justice get changed
in a way that he calls “seriously dislocating” and requires a significant
readjustment period (Dworkin 2002, 444). Dworkin argues that the reason our views on ethics and
justice get changed is because our ideas about responsibility depend on the
border between chance and choice. New scientific developments can change this
border. Similarly, the prospects of novel enhancements and modifications present
us with a “seriously dislocating” set of new decisions.
As Bostrom
and Ord point out, modification decisions are not the
only ones we have to make without sufficient information. Decisions about
careers, becoming parents, and getting married are all high stakes decisions
that we make without knowing whether they will turn out for the best (Bostrom and Ord 2006, 657). There is, however,
one key difference between, for example, the decision to become a parent and
the decision to adopt a radically new way of sensing the world. Many people
like us have become parents before. We do not have a guarantee that our choice
to become a parent will, on balance, be a good choice, but we do have access to
a reasonable amount of information about this choice. Until we get to Stage 3
with modifications, decisions about modifying ourselves in novel ways will not
be on a par with decisions about becoming parents or getting married or
selecting a career.
Where do we go from
here? Novel decisions are coming whether we like it or not. Marcus Arvan has an interesting answer, which he raises in the
context of discussing transformative choices such as whether to become a
parent. He proposes that instead of trying to fix the decision problem, we
should work on becoming more resilient people so that we can adapt fruitfully
to whatever outcomes arise (Arvan 2015).
While this sounds like sage advice, I am troubled by the thought that, should I
wind up making a modification that provides me with a negative WIILFA, I should
rest content with the knowledge that I am the kind of person who will make the
best of it. The bioconservative faces a similar
problem in resting content with the idea that, even if he avoided selecting a
beneficial modification, he should make the best of it. More disquieting is the
tacit admission that, because of our psychology and our lack of access to
information, we simply do not have a good decision toolkit available to
navigate the types of decisions we will soon be facing about how we want to
change our bodies and ourselves.
More promising are the
suggestions that we attend to prototyping and empirical evidence. Here are just
a few brief considerations. As already mentioned, not all aspects of a novel
experience can be prototyped. One point of concern is that it will be
particularly difficult to prototype duration (if the decider is considering a
permanent change, then this permanence cannot be prototyped in advance).
Another concern is that the prototype, by definition, will not be at the same level
of risk because prototyping involves making lower risk decisions in advance of
the higher risk decision. Finally, since some modifications can be more easily
prototyped than others, this might influence the direction of research on
modifications in much the same way that activity trackers that only measure
steps might encourage a focus on step-based exercise over other forms of
exercise.
When it comes to
relying on empirical evidence, one way to strengthen the analogy between the
early and late adopters (Stage 2 to Stage 3) is to introduce modifications
incrementally. The differences between early and late adopters need not be so
strong when the modification in question is a modest change. The worry, though,
is that, if we pursue this route, we are deciding not to pursue more dramatic
modifications at the moment, and this decision might be the wrong one. We might
be able to satisfy preferences about the WIILFA by rolling out modifications
quickly.
In this article, in
addition to focusing on decisions made about satisfying preferences about the
WIILFA, I have been focusing on individual decisions made in isolation. The
decisions others make will influence the calculation in a way that complicates
things tremendously. For example, those who get value from the novelty factor
will find out that the value of their modification decreases as others start to
adopt it. For another example, refusing a modification might initially be the
right move, but as others adopt it, a variety of pressures might be brought to
bear on the refuser that will change the values of
the outcomes. Consider the fact that it is increasingly difficult to navigate
our modern world without a cell phone, which puts pressure on people to
purchase one. Similar types of market and social forces could put pressure on
people to modify themselves, which could increase the costs of not modifying.
Ultimately, after considering ways to improve on the information we have to inform
our own individual decisions, we will need to turn to the herculean task of
sorting out rational decisions in a context where the decisions that others
make will influence which decisions are rational for us.
Notes
1. I am not staking a
claim on the nature of well-being by focusing on
preference satisfaction, because I am not claiming that satisfying preferences
is the key to well-being. Instead, I am simply focusing on the types of
decisions that appropriately depend on preference satisfaction. There are many
other types of decisions we might make, and some of those other types might be
instrumental in improving well-being.
2. Thanks to an
anonymous reviewer for this and many other insightful observations.
3. Rachel McKinnon
uses the convention “trans*” as an inclusive term referring to a variety of
transgender identities.
References
Agar, Nicholas. 2014. A question about defining moral
bioenhancement. Journal of Medical Ethics
40: 369–70.
Archer,
Alfred. 2016. Moral enhancement and those left behind. Bioethics 30: 500–510.
Arvan, Marcus. 2015. How to rationally approach life’s
transformative experiences. Philosophical
Psychology 28: 1199–1218.
Binmore, Ken. 2009. Rational
decisions. Princeton, NJ: Princeton University Press.
Bostrom, Nick, and Toby Ord. 2006. The reversal test: Eliminating
status quo bias in applied ethics. Ethics
116: 656–79 .
Bostrom, Nick, and Anders Sandberg. 2009. The wisdom
of nature: An evolutionary heuristic for human enhancement. In Human enhancement, ed. Julian Savulescu
and Nick Bostrom, 375–416. Oxford and New York: Oxford University Press.
Buchak,
Lara. 2013. Risk and rationality:
Oxford University Press.
Burnett, Bill, and David John Evans. 2016. Designing your life: How to build a
well-lived, joyful life. New York: Alfred A. Knopf.
Cabrera, Laura Y. 2011. Memory enhancement: The issues
we should not forget about. Journal of
Evolution and Technology 22(1): 97–109 .
Chatwin, Caroline, Fiona Measham, Kate O’Brien, and
Harry Sumnall. 2017. New drugs, new directions? Research priorities for new
psychoactive substances and human enhancement drugs. International Journal of Drug Policy 40: 1–5.
Coeckelbergh, Mark. 2011. Vulnerable cyborgs: Learning
to live with our dragons. Journal of
Evolution and Technology 22(1): 1–9.
Crittenden, Chris. 2002. Self-deselection:
Technopsychotic annihilation via cyborg. Ethics
and the Environment 7(2): 127–52.
Daniels, Norman. 2009. Can anyone really be talking
about ethically modifying human nature? In Human
enhancement, ed. Julian Savulescu and Nick Bostrom, 25–42 . Oxford and
NewYork: Oxford University Press.
Dougherty, Tom, Sophie Horowitz, and Paulina Sliwa.
2015. Expecting the unexpected. Res
Philosophica 92: 301–21.
Douglas, Thomas. 2015. The harms of enhancement and
the conclusive reasons view. Cambridge
Quarterly of Healthcare Ethics 24: 23–36.
Dworkin, Ronald. 2002. Sovereign virtue: The theory and practice of equality. Cambridge, MA:
Harvard University Press.
Edelman, Shimon. 2018. Identity, immortality,
happiness: Pick two. Journal of Evolution
and Technology 28(1): 1–17 .
Fukuyama, Francis. 2003. Our posthuman future: Consequences of the biotechnology revolution.
New York: Picador.
Gilbert, Daniel T., Matthew A. Killingsworth,
Rebecca N. Eyre, and Timothy D. Wilson. 2009. The surprising power of
neighborly advice. Science 323:1617– 619.
Graafstra, A.
2013.
Biohacking – the forefront of a new kind of human
evolution: Amal Graafstra
at TEDx SFU. YouTube video file, posted October 17,
2013. Duration 16:38. https://www.youtube.com/watch?time_continue=88&v=7DxVWhFLI6E (accessed May 7, 2019).
Harbisson, Neil, and Moon Ribas. 2018. Cyborg
Foundation, history.
https://www.cyborgfoundation.com/ (accessed June 6,
2018).
Hines, Alice. 2018. Magnet implants? Welcome to the
world of medical punk. New York Times.
May 12.
https://www.nytimes.com/2018/05/12/us/grindfest-magnet-implants-biohacking.html?hp&action=click&pgtype=Homepage&clickSource=story-heading&module=second-column-region®ion=top-news&WT.nav=top-news
(accessed May 21, 2018).
Hsee, Christopher K., Reid Hastie, and Jingqiu Chen.
2008. Hedonomics: Bridging decision research with happiness research. Perspectives on Psychological Science 3:
224–43.
Hurwicz, Leonid. 1951. Optimality criteria for
decision making under ignorance. Cowles Commission Discussion Paper, Statistics
no. 370.
Jeffries, Stuart. 2014. Neil Harbisson: The world’s
first cyborg artist. The Guardian.
May 6.
https://www.theguardian.com/artanddesign/2014/may/06/neil-harbisson-worlds-first-cyborg-artist
(accessed May 21, 2018).
Kahneman, Daniel. 1992. Reference points, anchors,
norms, and mixed feelings. Organizational
Behavior and Human Decision Processes 51: 296–312.
Krishnamurthy, Meena. 2015. We can make rational
decisions to have a child: On the grounds for rejecting L.A. Paul’s arguments. In
Permissible progeny?: The morality of procreation
and parenting, ed. Sarah Hannan, Samantha Brennan, and Richard Vernon, 170–83.
New York: Oxford University Press.
Lara, Francisco. 2017. Oxytocin, empathy and human
enhancement. Theoria: An International
Journal for Theory, History and Foundations of Science 32: 367–84.
Heath, Chip, Richard Larrick, and George Wu. 1999.
Goals as reference points. Cognitive
Psychology 38: 79–109.
Liao, S. Matthew, Anders Sandberg, and Rebecca Roache.
2012. Human engineering and climate change. Ethics,
Policy & Environment 15: 206–21.
Madrigal, Alexis. 2016. I got a magnet implanted into
my finger for science, and it was amazingly weird. Splinter. April 6.
https://splinternews.com/i-got-a-magnet-implanted-into-my-finger-for-science-an-1793856036
(accessed May 18, 2018).
Martens, Rhonda. 2016. Resource egalitarianism,
prosthetics, and enhancements. Journal of
Cognition and Neuroethics 3(4): 77–96.
Mather, Mara, and Marcia K Johnson. 2000.
Choice-supportive source monitoring: Do our decisions seem better to us as we
age? Psychology and Aging 15: 596–606.
Mather, Mara, Marisa Knight, and Michael McCaffrey.
2005. The allure of the alignable: Younger and older adults’ false memories of
choice features. Journal of Experimental
Psychology: General 134: 38–51.
McKinnon,
Rachel. 2015. Trans*formative experiences. Res
Philosophica 92: 419–40.
Mihailov, Emilian, and Alexandru Dragomir. 2018. Will
cognitive enhancement create post-persons? The use(lessness) of
induction in determining the likelihood of moral status enhancement. Bioethics 32: 308–313.
Paul, L. A.
2014. Transformative experience.
Oxford: Oxford University Press.
Paul, L. A. 2015a. Transformative choice: Discussion
and replies. Res Philosophica 92: 473–545
.
Paul, L. A. 2015b. Transformative experience: Replies
to Pettigrew, Barnes and Campbell. Philosophy
and Phenomenological Research 91: 794–813.
Paul, L. A. 2015c. What you can’t expect when you’re
expecting. Res Philosophica 92: 149–70.
Persson, Ingmar, and Julian Savulescu. 2013. Getting
moral enhancement right: The desirability of moral bioenhancement. Bioethics 27: 124–31.
Pettigrew, Richard. 2015. Transformative experience
and decision theory.
Philosophy and
Phenomenological Research 91: 766–74.
Sample, Ian. 2006. Man rejects first penis implant. The Guardian. September 18.
https://www.theguardian.com/science/2006/sep/18/medicineandhealth.china
(accessed May 18, 2018).
Sandel, Michael J. 2009. The case against perfection. Cambridge, MA: Belknap Press.
Savage,
Leonard J. 1972. The foundations of
statistics. Second ed. New York: Dover.
Skyrms,
Brian. 1990. The dynamics of rational
deliberation. Cambridge, MA: Harvard
University
Press.
Stix, Madeleine. 2016. World’s first cyborg wants to
hack your body. CNN. January 7.
https://www.cnn.com/2014/09/02/tech/innovation/cyborg-neil-harbisson-implant-antenna/index.html (accessed May 9, 2019).
Stoll Benney, Kristen, and Linda A. Henkel. 2006. The
role of free choice in memory for past decisions. Memory 14: 1001–1011.
Stoye, Jörg.
2011. Statistical decisions under ambiguity. Theory and Decision 70: 129–48.
Torres, Phil. 2016. Agential risks: A comprehensive
introduction. Journal of Evolution and
Technology 26(2): 31–47.
Wald,
Abraham. 1950. Statistical decision
functions. New York: Wiley.
Walsh, Emma, and Peter Ayton. 2009. My imagination versus your
feelings: Can personal affective forecasts be improved by knowing other
peoples’ emotions? Journal of Experimental Psychology: Applied
15: 351–60.
Weirich, Paul. 2004. Realistic decision theory: Rules for nonideal agents in nonideal
circumstances: New York: Oxford University Press.
White, Amy. 2014. Body integrity identity disorder
beyond amputation: Consent and liberty. HEC
Forum 26: 225–36.
Whitmore, G. A., and M. C. Findlay. 1978.
Introduction. In Stochastic dominance: An
approach to decision-making under risk, eds G.A. Whitmore and M.C. Findlay,
1–36. N.p.: D.C. Heath.
Wilson, Timothy D., and Daniel T. Gilbert. 2005.
Affective forecasting: Knowing what to want. Current Directions in Psychological Science 14: 131–34.